Hysterectomy Q&A with Dr. Litrel
Dr. Litrel addresses the most frequently asked questions about hysterectomies. Watch more GYN Problems videos below
Dr. Litrel addresses the most frequently asked questions about hysterectomies. Watch more GYN Problems videos below
by Michael Litrel, MD, FACOG, FPMRS When my son Tyler was fifteen, I brought him with me on a church mission trip to Honduras. It seemed an inspired idea: I was seized with a vision of him forsaking his Xbox for a transformative week of caring for poor people in a third world country. Twenty of us boarded the plane headed for rural Central America. Our physical task was to repair homes. Our spiritual task was to learn and teach about God’s love. Tyler was shocked by the poverty. Forty people lived in the remote village in mud and stick huts. They had no running water or electricity. Wandering the village were dogs so emaciated you could count each rib. Over the days that followed, Tyler took me to the side several times to sort through his feelings. How could we have so much at home when others in the world have so little? I was proud of him, growing up, asking the right questions… But as it turned out, he was still an obtuse adolescent. On the last day, we faced a grueling three-mile hike through the steaming jungle to the work site. Tyler assured me he had filled all our water bottles. But when we arrived, I discovered only three of the eight bottles were full. Tyler had gotten lazy and just hadn’t bothered. I was livid. We had an entire afternoon of physical labor ahead. Don’t you realize we have four THOUSAND pounds of cement to mix? How can we work without water? Blah, blah, blah… I’m sorry, DAD!!! I GET it! Tyler threw up his hands in exasperation. I could tell Tyler was more angry than sorry. But I stopped and sulked away, muttering dark thoughts under my breath. I had been proud that Tyler had chosen to come – the youngest in the group by five years. Heaven knows it was gratifying to see his hands finally off the game controller and wielding a shovel full of dirt. But I didn’t want to hear any adolescent fibs about filling water bottles. Our project was a hut with a dirt floor, to be replaced with cement. Twenty bags of mix had already been carried to the site. The choice of tasks were these: carry buckets of water from the stream, mix the cement on the ground, carry the wet cement into the hut, or lay down the floor. There were eight of us. It was back-breaking work. Three hours later, we lay exhausted under the hot equatorial sun. A feeling of discouragement began to creep over us. The floor was only a third done, and we were running out of both cement and energy. I slumped on a stool. A small village girl named Amalia crept quietly next to me. Her dress was worn, her face dirty, but her smile was glowing. She was one of eight children who lived in this tiny hut. A cement floor would keep her young body off the ground at night. Tyler rested motionless, his back against a tree. His work efforts had been listless at best. But I kept my criticism to myself. At least he was here. Just when the job seemed hopeless, a few neighboring villagers arrived to help. Recharged, we resumed mixing cement, carrying bucket after bucket into the hut. Somehow, we now had so much that we could not only cover the entire dirt floor but even make a front porch. Remarkably, too, our water bottles never ran out. Tyler and I had enough to last all afternoon. It was a strange and wonderful day in Honduras. Tyler and I had partaken in a kind of miracle: plenty of cement, a floor for Amalia, and even enough water. For me, it was a spiritual reminder that we are always given enough – an ironic lesson to learn while helping a family whose belongings could fit in the trunk of my car. It was only later, as I was falling asleep, that I figured out – Tyler had left all the water for me. Excerpted from Dr. Litrel and his wife Ann’s book of “he-said, she-said” stories about love and family. A MisMatch Made In Heaven: Surviving True Love, Children, and Other Blessings In Disguise is available in the office, and online at www.createspace.com/4229812

If you have a history of painful periods, pain with sex, or general pelvic pain, there is a good chance you have endometriosis. Endometriosis is a condition that affects over six million women and teens in the United States, and millions of other women worldwide. Causes and Symptoms of Endometriosis While the definite causes of endometriosis aren’t 100% clear, possible causes include: Retrograde menstruation Embryonic cell growth Surgical scar implantation Endometrial cells transport Immune systems disorder Symptoms can be varied, with some women experiencing little to no pain and others experiencing moderate to heavy amounts of pain during periods, sexual intercourse or with bowel movements. Other symptoms include: Fatigue Diarrhea Constipation Bloating Nausea Excessive bleeding Infertility Treatment Strategies for Endometriosis While there is not a cure for endometriosis, certain treatment options can help with pain and infertility. Treatment will vary depending on your symptoms, your age, and whether or not you have future plans of becoming pregnant. Medication – Over-the-counter pain relievers may include aspirin and acetaminophen, as well medicines that inhibit prostaglandin (the hormone that controls processes such as inflammation, blood flow, and the formation of blood clots and the induction of labor). These include ibuprofen and naproxen sodium. If pain is very severe, prescription drugs may be required. Hormonal Therapy – Hormonal treatment aims to stop ovulation for as long as possible and may include: oral contraceptives, progesterone drugs, a testosterone derivative (danazol), and GnRH agonists (gonadotropin releasing hormone drugs). Side effects may be a problem for some women. Surgery – If your doctor has determined that surgery is the best treatment option, a board-certified FPMRS (Female Pelvic Medicine and Reconstructive Surgeon) can determine what surgical method works best for your needs. FPMRS surgeons are highly skilled in the diagnosis, evaluation and both surgical and non-surgical treatment of pelvic floor disorders such as endometriosis. Types of Surgery For Endometriosis A more conservative surgery option consists of using a laparoscope to find and remove any growths to remove pain and increase the possibility of pregnancy. In some cases, hormonal therapy may be prescribed in conjunction with conservative surgery. In more severe cases, your surgeon may recommend a hysterectomy, removal of all growths, and removal of ovaries (also called oophorectomy). These types of surgeries are considered only when other treatment options have offered little relief, as the surgery causes early menopause. Additionally, it is only considered when you have no future plans to become pregnant. The OB/GYNs at Cherokee Women’s have a deep understanding of women’s anatomy and the types of concerns that women struggling with endometriosis may be facing. Our board-certified FPMRS doctors can address concerns related to scar tissue, internal trauma after childbirth, excessive bleeding and infertility. If you have questions or concerns regarding symptoms or treatment for endometriosis, don’t hesitate to schedule an appointment.

The Centers for Disease Control made headlines this week when they announced that sexually active women of childbearing age should never drink alcohol unless they’re on birth control. The recommendation met with both support and backlash: many women agree that it’s not worth the risk, while others argue that telling 3.3 million women not to drink isn’t feasible. What do you think? Are You Expecting? You probably know that consuming alcohol during pregnancy can negatively impact a baby’s mental, physical, and behavioral development. What you may not know is whether or not you’re expecting. Some moms-to-be take 4 to 6 weeks to realize they’re pregnant. And as many moms of lovable broods know, about half the pregnancies in the United States are unplanned. Even women actively trying to get pregnant might continue drinking. According to the CDC, only 1 in 4 women stops drinking alcohol when they go off birth control. Exposure to even minimal alcohol during pregnancy may affect the baby’s health. So is the risk worth it? The Effect of Alcohol on Developing Babies Whether you’re happily expecting or simply trying, we know your baby’s health is your #1 consideration. But you may not realize just how much damage drinking during pregnancy can cause. Even small amounts of alcohol can cause: Miscarriage Stillbirth Prematurity Fetal Alcohol Spectrum Disorders (FASDs) Sudden Infant Death Syndrome (SIDS) FASDs can affect a child’s development both before and after birth. Symptoms can include anything from abnormal facial features and underdeveloped growth to poor memory, attention or hyperactivity disorders, learning disabilities, speech and language problems, and low IQ. Many people suffering from FASDs also have impaired hearing or vision and problems with their hearts, kidneys, or bones. Make the Healthy Choice At Cherokee Women’s Health, we advocate for the health of mothers and their babies. According to the CDC recommendation, all expectant mothers should refrain from drinking alcohol during pregnancy. If you’re trying to get pregnant, we recommend that you stop drinking alcohol until you go back on birth control. If you discover you’re pregnant unexpectedly, stop drinking immediately. Cherokee Women’s Health has an experienced team of obstetricians, dedicated nurse-midwives, and board certified FPMRS surgeons on staff. We specialize in normal and high risk pregnancies, with expert care physicians and advanced practice providers trained in both natural and standard births. To learn more about how to ensure a healthy pregnancy, call today or schedule an appointment online.

When you’re diagnosed with pelvic organ prolapse, you’re faced with a challenging and emotionally painful question: Should I continue adding children to my family? Whether you’ve always wanted a big family, or just two children, you know that your health is in a precarious and delicate state. You’re afraid of worsening your prolapse, but even more afraid that you will regret not choosing to become pregnant again. Talking with a urogynecologist who specializes in Female Pelvic Medicine and Reconstructive Surgery may help to make this decision easier for you to make. Since there are surgical and non-surgical treatment options for any stage of prolapse, your doctor can offer insight that may alleviate your fears and concerns. Once you’ve settled on an additional pregnancy, it is important to take care of yourself physically in order to optimize a birth and post-partum period that will accommodate your body and your prolapse. Pelvic organ prolapse doesn’t have to rule your decisions. Don’t let your limitations hold you back from living the life you want. During and After Pregnancy Prolapse Care Pelvic Floor Physical Therapy – The exercises and touch therapy included in PT can help to keep your symptoms to a minimum throughout your pregnancy. Ask your urogynecologist or OB/GYN for a referral to a physical therapist who specializes in women’s health. After you deliver, check with your urogynecologist and OB/GYN to be cleared to begin the healing process of post-partum physical therapy. Prenatal and Post-Partum Support – When worn correctly, a maternity belt can ease pressure on the pelvic floor and lower back, allowing you to move easier and prevent straining. Different from a waist-trainer or girdle, effective post-partum support can be therapeutic for a healing pelvic floor. Run these products by your doctor to see if they will work for you and your limitations. Conscientious Movement – Remember that you are growing a baby, as well as nursing your prolapse. Move with purpose, and don’t push yourself to the point of pain. Lifting should be kept to a minimum, as well as bending over. When you do have to make larger movements, engage your transverse abdominus and kegel muscles. Keeping theses muscles strong will help support your pelvic floor, and help prevent any stress urinary incontinence. When recovering from birth, give yourself time to heal. Move slowly, and deliberately, and “baby” your pelvic floor. Ask your doctor how soon you can resume any pelvic floor exercises, and start slowly, working yourself up to your pre-pregnancy status. Simple life adjustments can have a big impact on a successful pregnancy and post-partum period. Cherokee Women’s Health Can Help Our board-certified physicians are female pelvic health experts and can help. Call us today at 770.720.7733 or schedule an appointment online.

Pain, pressure, and fullness are very common complaints during pregnancy. But when those pesky symptoms don’t subside after birth, you may be dealing with pelvic organ prolapse. Pelvic organ prolapse, or POP, occurs when your pelvic floor suffers damage from pregnancy and childbirth. The weight of carrying your baby for nine months, as well as a difficult or traumatic birth, can tear the ligaments and connective tissue of your pelvic floor. As a result, your injured pelvic floor may have difficulty holding your organs — such as your uterus, intestines, rectum, urethra, and bladder — in place, and they fall downward. Symptoms of Pelvic Organ Prolapse Include: Urinary issues such as incontinence or difficulty urinating Bowel movement issues such as constipation or straining to use the bathroom Painful sex or intercourse Lower back pain. POP is usually diagnosed after birth when the symptoms persist; the complications can range from mild to severe. Every prolapse is different and will require a specialist’s approach in both diagnosing and treating your prolapse. Though childbirth is the most common reason women develop POP, there are other risks that make a woman prone to the condition. Common Causes of POP Include: Childbirth Genetics Smoking Chronic coughing Straining Heavy lifting Menopause Obesity Nerve or muscular damage. Help is Available If you experience any symptoms related to pelvic organ prolapse, or want to discuss risk factors, schedule an appointment today. If you do have POP, there are options available to you so that you don’t have to endure the effects of your prolapse long-term. Our double board-certified urogynecologists specialize in Female Pelvic Medicine and Reconstructive Surgery and can assist you in choosing the right treatment plan for you. POP doesn’t have to rule your life. Call us today at 770.720.7733 or schedule an appointment online.

If you have pelvic floor dysfunction, this may be one way you might describe your symptoms. Other ways to describe it may include: A strange, new sensation has taken over your body. Simply put into words: it feels like your bottom is falling out. You may be hesitant to share this information with just anyone, but you can’t help but wonder what could be causing this unsettling symptom. Women who suffer from pelvic floor dysfunction have used this description and the others above to explain exactly what is happening down there. Pelvic floor dysfunction, or PFD, is a set of conditions that cause women to experience unpleasant urinary and bowel disorders or pelvic organ prolapse, also known as POP. Symptoms of these disorders include urinary or fecal incontinence, pain, pressure, or constipation. So, how exactly did your bottom end up this way? Over time, your pelvic floor muscles have endured some damage or weakness that has caused your organs to sag into your vagina, or rectum, hence the feeling that something is “falling out”. Childbirth is a very big factor that plays into PFDs, but there are other causes as well including genetics, heavy exercise, straining, and other health impairments. Every woman has a different experience with PFD and you should always keep this in mind when discussing treatment plans with your doctor. The effects of PFD can range from mild to severe, but there are treatment options that may work for you. Sometimes treatment includes simple lifestyle changes, physical therapy, an intravaginal device called a pessary, or surgery, including the placement of transvaginal mesh. Take back your body! Make an appointment with one of our board-certified female pelvic medicine and reconstructive surgery specialists to start the conversation about PFD. Call us at 770.720.7733 or schedule an appointment online.

Sometimes suffering with pelvic floor dysfunction, or PFD, can make you feel like you are limited in what you can do. If you’ve been diagnosed with pelvic organ prolapse, urinary incontinence, or bowel control issues, it can be confusing or frustrating for you as you try resuming your normal daily routine without irritating your symptoms. Being able to lead a full, satisfying life with PFD is important, but engaging in activities which aggravate your disorder can cause your symptoms to worsen. Here are some things to keep in mind about PFD as you go about your daily life. 1. DO Exercise Don’t choose a workout that includes heavy-lifting such as crossfit, or will put intense pressure on your pelvic floor such as running, or plyometrics. The straining in those types of activities can cause your PFD to get worse over time. Choose exercises such as restorative yoga, walking, and other low impact exercise that will not put pressure on your pelvic floor. Looking for something specific? Check out Hab-It, or Pfilates™ 2. DO Pelvic Brace Don’t forget to engage your transverse abdominus (your lower abdomen) and your Kegel muscles when you sneeze, cough, or laugh can cause urine leakage to occur. Brace yourself and save a trip to the bathroom and a change of underwear. When you engage these muscles, your pelvic floor will not feel the downward pressure that results from these everyday movements. 3. DO Retrain your Bladder Don’t head to the bathroom every time you feel the slightest urge to pee. Your bladder needs retraining to stop triggering frequent restroom breaks out of habit. To start retraining, avoid taking bathroom trips less than two hours apart. Over time, you will you find that you have the urge to urinate less frequently and you will be urinating larger amounts. Not sure if you’re releasing a full bladder? Count how long you urinate for. A full bladder should be a stream of at least ten seconds long. Don’t forget to count with a “Mississippi” in between each number! Tell your bladder who’s in control and retrain yours! 4. DO Seek Treatment Don’t suffer from the interfering symptoms of PFD. There are treatment options available that will fit your lifestyle and diagnosis. The first step is finding a urogynecologist who can assess your needs and suggest a treatment that will work for you. Some of those choices may include: physical therapy, pessaries, medicines, or surgery. 5. DO Live Your Life Don’t let your PFD slow you down or dampen your spirits. Modify your activities, but not your life to adjust to your diagnosis. Consider joining an online support group to help you cope with the struggles of PFD. Visit voicesforpfd.org for more information about how you can reach out to others who are suffering from PFD, as well. Cherokee Women’s Health Can Help Our board-certified physicians are female pelvic health experts and can help. Call us today at 770.720.7733 or schedule an appointment online.

Cherokee Women’s Health celebrates American Heart Health Month. After all, moms-to-be aren’t just keeping one heart healthy. From the first time you hear your baby’s heartbeat, your own is racing with anticipation, joy, and more than a few nerves. Keep your heart strong during pregnancy by taking care of your body and your health. Eat High Fiber Grains and Nuts Get plenty of omega-3 fatty acids from olive oil and pregnancy-safe fish like salmon Avoid salt, which can increase blood pressure Do several low-to-moderate intensity workouts each week, unless your doctor recommends rest Avoid eating or drinking caffeine, which can cause irregular heartbeats Avoid Consuming Caffeine Caffeine increases your blood pressure and heart rate — bad news for both your pregnancy and your heart health. Not only can it lead to dehydration, caffeine crosses the placenta to your baby, who can’t yet metabolize it . Most women know to avoid major sources of caffeine like coffee during pregnancy, but you may not realize how many of your favorite craving snacks sneak caffeine into the mix. Caffeine is found in: Tea Soda Coffee (even decaf!) Chocolate Energy-enhancing foods and drinks (such as energy water or fortified foods) Coffee or chocolate flavored ice cream Some over-the-counter pain relievers like Excedrin While it’s considered safe to consume small amounts of caffeine during pregnancy, it’s easy to lose track. Talk to your doctor about how much caffeine is safe for you and your baby during your pregnancy. Heart Disease and Pregnancy If you’ve ever been diagnosed with heart disease, high blood pressure, or have had cardiac symptoms such as chest pain, shortness of breath or palpitations, alert both your cardiologist and your OB/GYN. List all medications you’re taking, and make sure none of them will have adverse side effects on your baby’s development. For more information on health during pregnancy, contact Cherokee Women’s Health at 770.720.7733 or schedule an appointment online today.
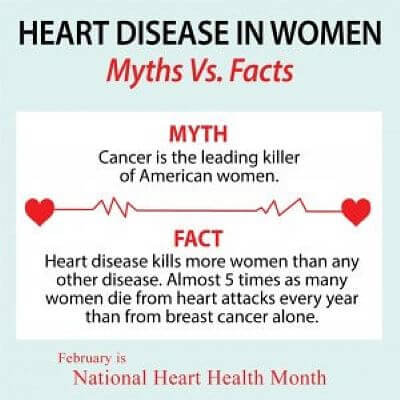
Did you know heart disease is the No. 1 killer of women, causing 1 in 3 deaths each year? That’s approximately one woman every minute so it’s important to know the symptoms and how you can take control of your risk factors. The Most Common Heart Attack Symptoms in Women Shortness of breath Uncomfortable pressure, squeezing, fullness or pain in the center of your chest. Nausea, vomiting, cold sweat or lightheadedness Pain or discomfort in any of the following: jaw, neck, stomach, arms (one or both). Lifestyle Changes to Help Prevent Heart Disease There are many things you can do to control heart disease and with the right information and care, heart disease in women can be treated, prevented and even ended. Studies show that healthy choices have resulted in 330 fewer women dying from heart disease per day. Don’t smoke Manage your blood sugar Get your blood pressure under control Lower your cholesterol Know your family history Stay active Lose weight Eat healthy Trust your gut Women are less likely to call 9-1-1 when experiencing symptoms of a heart attack themselves so trust your gut. If you aren’t feeling normal or are experiencing any of the symptoms above, call 911 or head to your local emergency room.

Dr. Sara Bolden is a women’s health physical therapist, board-certified women’s health clinical specialist, owner of Women First Rehabilitation in Woodstock, GA and author of What a Girl Wants: The Good Girl’s Guide to Great Sex. Adopting a Higher Quality Obstetrical Care Model for Women in the United States If you’ve ever had a baby, witnessed one being delivered or heard of someone’s detailed labor and delivery story, one thing’s for sure, there was pain involved. We’re not talking about a little discomfort here, folks. We’re talking about deep, intense, I-could-kill-the-man-that-did-this-to-me pain. Quite honestly, we’ve come to expect extreme bodily pain during a situation like this. It would be absolutely crazy to think otherwise. I mean, we’re talking about a small melon exiting out of an opening the size of a child’s sock. Yes, the sock will stretch, the melon will emerge, but not without some repercussions…sometimes big repercussions. Often, these consequences can be serious and have lasting musculoskeletal effects. So what’s a girl to do? Physical Therapists Are NOT Massage Therapists Many would say, childbirth trauma is inevitable so proverbially “push” through the pain and try to get over it quickly. Unfortunately, this is frequently the default response to childbirth in the United States. There is little to no preparation of the pelvic floor muscles, the low back, the abdomen, nor education for proper breathing, delivery positioning, energy conservation or anything, for that matter, that adequately prepares the body’s musculoskeletal system for the delivery of a small human being. However, for many years now, international countries, such as England, Germany, Australia, Brazil and South Africa (to name a few), have taken proactive measures to assist women with labor and delivery and thus lower the risk of long-term musculoskeletal injuries or urogenital dysfunctions. One way they have elevated the standard of obstetrical care is to include physical therapists throughout pregnancy, during labor/delivery and for postpartum recovery. You might be saying to yourself, “physical therapists? Don’t they just give massages?” Brace yourselves…wait for it…no, they don’t. Physical therapists are not massage therapists. They are, however, musculoskeletal experts that have unique knowledge of the evaluation, assessment, treatment, disease/injury prevention and general wellness of the human body. The Difference a Women’s Health Physical Therapist Makes In other countries, the physical therapists that assist with prenatal and postpartum women are called obstetrical physiotherapists and have advanced skill and training in women’s health. In the United States, we call them women’s health physical therapists. I know, ingenious. They, too, have advanced knowledge and extensive training in women’s health; however in the U.S., their services have only been considered for the prenatal patient with abnormal or life-altering pain or for the complicated postpartum patient with pain and/or pelvic floor dysfunction (i.e. urinary incontinence, organ prolapse or pain with intercourse). Higher Standards of Obstetrical Care If the U.S. adopted a more comprehensive standard of obstetrical care, every pregnant women would be evaluated by a women’s health physical therapist. During the prenatal phase, she would get education and training on pelvic floor stabilization, core strengthening, body mechanics, birthing positions, perineal massage, breathing, relaxation and proper Valsalva for effective pushing, etc. Then, a women’s health physical therapist would be included in the delivery room to help with pain management, assist with birthing positions that open the pelvis and decrease risk of vaginal tearing, perform perineal massage to allow adequate room for the decent of baby, provide biomechanical support and coach the patient on the when’s and how’s of proper pushing…just like obstetrical physiotherapists are doing right now in other countries! After the birth of the baby, postpartum women would follow up with their women’s health physical therapist to assess healing of vaginal and/or abdominal tissues, be educated on scar management and facilitated tissue recovery, learn mechanics for lifting baby as well as for breastfeeding and restoring pelvic strength. Of equal importance, women’s health physical therapists would help new moms get their bodies back in shape, set realistic goals and expectations of motherhood and restore her vibrant, sexual health. Yes, I said “vibrant!” Who wouldn’t want that?! Good news! You belong to a cutting-edge OB/GYN practice and are hearing about women’s health physical therapists! I invite you to do a little research and see for yourself how effective this type of physical therapy is for pregnancy, labor, delivery and postpartum. Don’t be shy: ask your doctor to include physical therapy as part of your prenatal and postpartum experience. Company Bio Women First Rehabilitation is an elite healthcare practice devoted exclusively to treating individuals with pelvic pain, urogynecologic disorders and pelvic floor dysfunction in all phases of life. All of our practitioners are licensed women’s health physical therapists with advanced knowledge and training in women’s health. For more information, visit www.WomenFirstRehab.com.
For ten years, without fail, Ann and I kept our razors side by side in the shower. Then I switched to the Mach 3 triple blade razor, and suddenly the ever-present disposable pink lady razor disappeared. I didn’t give it much thought at the time. I figured such a sissy razor was an embarrassment beside my macho marvel of modern technology. The truth was more horrific. One morning I walked into the bathroom while Ann was in the shower, and I discovered that my Mach 3 triple blade marvel was being used to shave her legs. It didn’t take much to surmise that it might be getting some time under her arms, too. I kept my mouth shut until our morning coffee. “Doesn’t it repulse you,” I said calmly, “to know that the razor you’re using under your arms is the same one that I’m using on my face?” Ann laughed, and then quickly reached for my hand. “Sometimes…” she replied with a serious voice. “But love is a strange and wonderful thing.” She gave me an angelic smile. All was forgiven. Disagreement between a husband and wife occurs in the best of marriages. Sometimes this manifests as open argument. Other times, marital conflict can be more subtle, an unspoken tension permeating the relationship for years, like an uncomfortable humidity. When I met Ann at that fraternity costume party, she was supposedly dressed as a Greek goddess, in a skimpy toga no father would have permitted his daughter to wear in public. I fell in love. After our three years apart, there was nothing I looked forward to more than marriage and spending my life with Ann. My attraction to her was more than just her physical beauty; I admired her talent, kindness, intelligence and discipline. I still admire her. But after twenty-five years of marriage, the intelligence and discipline thing sometimes gets on my nerves. Ann has tendencies towards frugality that do honor to her Scottish heritage. She also endeavors to be environmentally aware. These two qualities are evidenced in the temperature settings Ann prefers for the household thermostat. During the hot Georgia summer the air conditioning is set at 80. During the cold of winter the heat is set at 65. In January when I am cold, Ann tells me to put on a sweater. In July when I am hot, Ann tells me to take my sweater off. Last year it was another hot, humid summer. So one day when Ann wasn’t looking, I sneaked to the thermostat and deftly dropped the temperature five degrees. It didn’t take Ann long to notice. “Who turned the air conditioning so low, Michael?” “Those kids,” I responded, shaking my head disapprovingly. I was not lying. I was simply making a declarative statement designed to misdirect. “The boys say they didn’t touch the thermostat, Michael.” “Those kids,” I repeated, shaking my head disapprovingly. Ann laughed and moved the thermostat back to “where it belongs.” I didn’t argue. I could understand her perspective: why burn fossil fuels to lower the temperature of my house just so I could be a tad bit more comfortable? But sometimes it was annoying. It was like I was married to Al Gore, and every time I touched the temperature control I was sinking an axe into the trunk of the last giant redwood. Over the years, Ann had successfully colored our “thermostat decision” in spiritual terms. With artful language she conveyed to me sophisticated thoughts about the needs of the body versus the needs of the soul. Essentially, her argument boiled down to this: Jesus didn’t have air conditioning, so why don’t you spend more time praying for strength, and less time whining about the heat? One summer Ann left town to visit her sister for a week. It was like Dorothy’s house had plopped down in Oz, and ding dong, you-know-who was dead! I ran to the thermostat like an unsupervised teenager and lowered it not five degrees, but ten. I was going to get all the air conditioning that compressor could muster. That night my house was so cold I needed another blanket from the closet. Immobilized by comforters, I slept like it was the dead of winter. Condensation covered all my windows when I awoke. I shivered when I sat down to my morning coffee. Now this was what July in Georgia should feel like! I thought about getting out that dang sweater. Maybe I should light a fire too? But after an hour of reflection, I simply turned the air conditioning off. I missed Ann. Morning coffee was more fun with her. It’s far better to have a home that is too hot in the summer and too cold in the winter than to suffer again through the fires and chills of a long distance relationship. A prescription for tolerance is an occasional few days apart. In our human struggles, we can sometimes fixate on small problems. Absence gives God a chance to direct our focus on the big picture – Love. Excerpted from Dr. Litrel and his wife Ann’s book of “he-said, she-said” stories about love and family. A MisMatch Made In Heaven: Surviving True Love, Children, and Other Blessings In Disguise is available in the office, and online at www.createspace.com/4229812
