Stages of Pregnancy – First Trimester
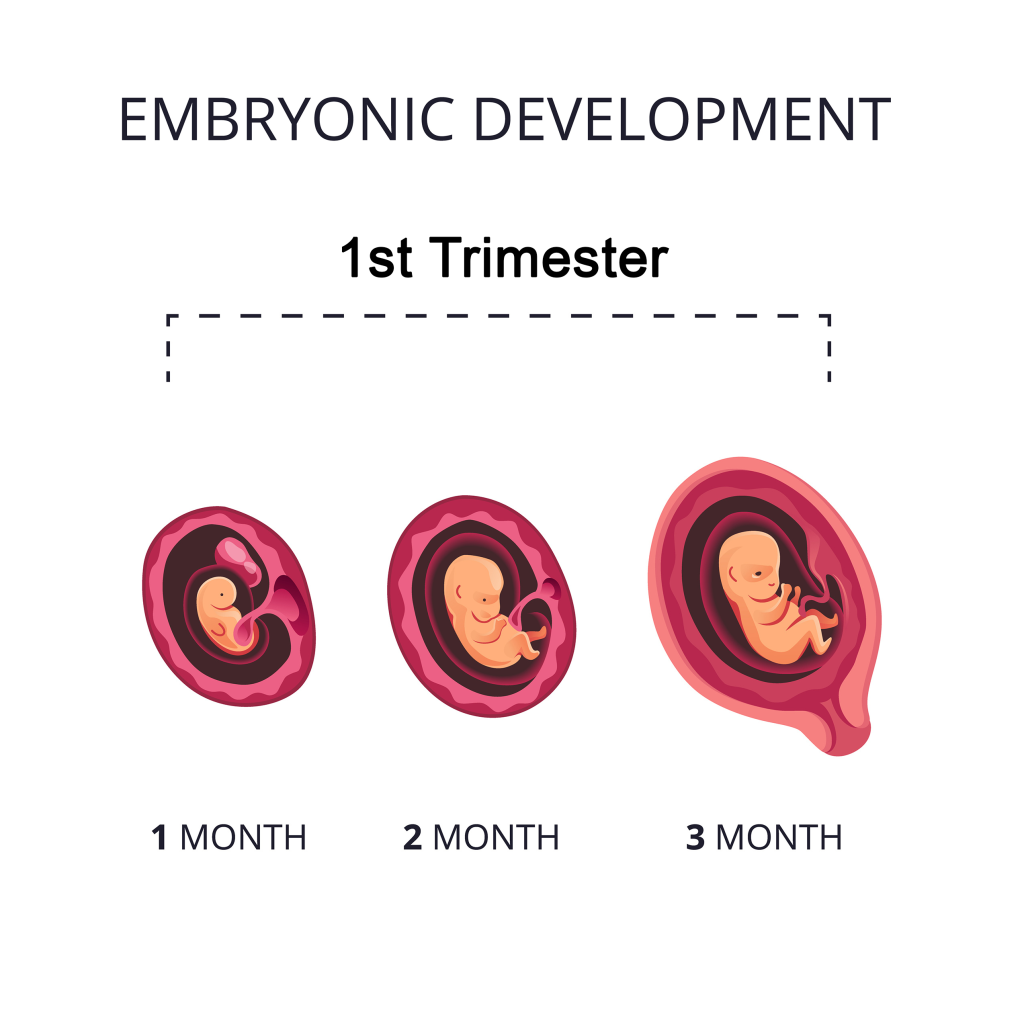
You’re in your first trimester — what an exciting time! Your body will go through many changes but don’t worry, we’ll explain everything to you in this 3-part series, from the first trimester through delivery. A “normal”, full-term pregnancy is 40 weeks and can range from 37 to 42 weeks. These stages are divided into three trimesters, each lasting about three months. The First Trimester – What is it and How Long Does it Last? The first trimester begins on the first day of your last period and lasts the first three months. This stage is crucial to the normal development of the fetus. While you may not be showing much on the outside, your body is doing miraculous things and your body and the fetus is changing rapidly. During the first trimester, your major body organs and systems of the fetus are forming. Weeks 3-10 is known as the organogenesis process. This is also when the fetus is most susceptible to damage from substances like alcohol, drugs and certain medicines, as well as illnesses such as rubella, also known as German measles. Fetus Growth and Development Even though you can’t see major changes on the outside, your baby is experiencing huge milestones in the first trimester. In fact, the fetus develops from a single fertilized cell (zygote) to a lemon-sized fetus of growing limbs and organs. The neural tube that is forming his or her spinal cord and brain is in place and by week 8, the brain will start moving those tiny, developing limbs. Other first trimester development milestones include: The End of Your First Trimester Around 12 weeks, nearly the end of your first trimester, your baby is about three inches long and weighs nearly an ounce. The head is much larger than the body and the brain and spinal cord are developing rapidly. Sex organs are forming, and while it is still too early to see the gender on the ultrasound, a genetic test can be ordered during this time, which can include the sex chromosomes. Your baby is now able to open and close his or her mouth and even make a fist. The baby is moving freely in the amniotic sac, although you can’t feel the kicks just yet. First Trimester Changes to Your Body It’s common for women to experience nausea during the first trimester. And while it’s most commonly known as morning sickness, it can occur at any time of the day. Every pregnancy is different. Some women have food cravings, others experience food aversions, while yet others may have no change in appetite at all. Physical Changes include larger, heavier and tender breasts. The uterus is also expanding which puts pressure on your bladder, resulting in having to urinate more often. Emotional Changes Emotions are in full swing during the first months of pregnancy. Hormone changes may make you feel irritable or moody, and tiredness is also very common in the early months. Know that these feelings, while new to you, are completely normal. However, if you are feeling extremely anxious or down, please speak with your physician or midwife. We are here for you! Learn what to expect during your 2nd trimester and 3rd trimester.