Wonderful Testimonial
I received this wonderful handwritten card from my patient Steffanie. She also gives thanks to our great staff. It is humbling when our patients take time out of their busy days to let us know that we made a difference.
I received this wonderful handwritten card from my patient Steffanie. She also gives thanks to our great staff. It is humbling when our patients take time out of their busy days to let us know that we made a difference.
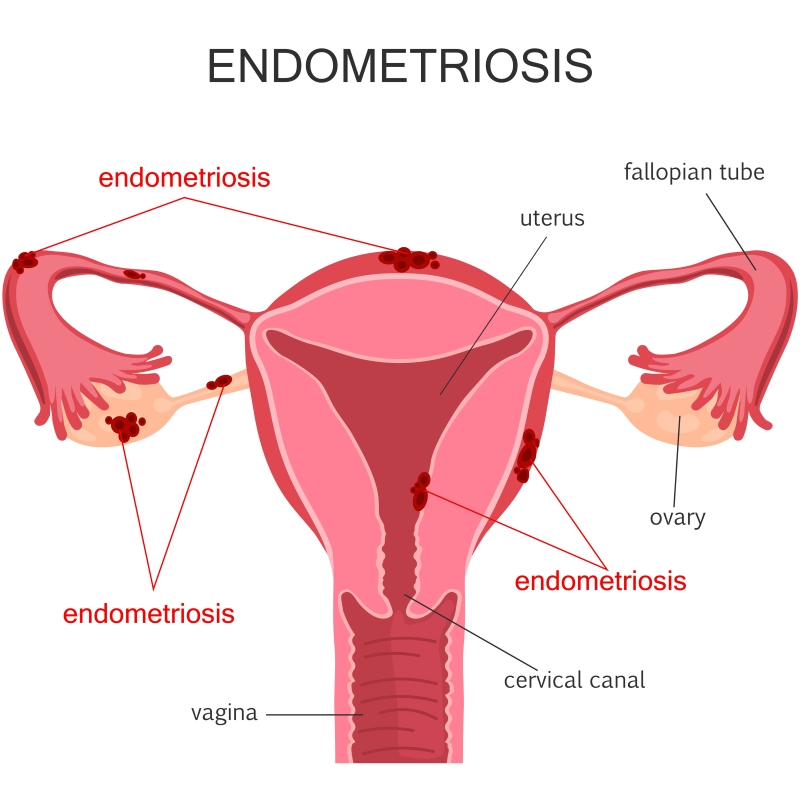
Endometriosis affects about 5 million American women. It’s an often painful disorder in which tissue that normally lines the inside your uterus — the endometrium — grows outside your uterus (endometrial implant). Endometriosis most commonly involves your ovaries, bowel or the tissue lining your pelvis. Rarely, endometrial tissue may spread beyond your pelvic region. In endometriosis, displaced endometrial tissue continues to act as it normally would — it thickens, breaks down and bleeds with each menstrual cycle. Because this displaced tissue has no way to exit your body, it becomes trapped. When endometriosis involves the ovaries, cysts called endometriomas may form. Surrounding tissue can become irritated, eventually developing scar tissue and adhesions — abnormal tissue that binds organs together. Endometriosis can cause pain — sometimes severe — especially during your period. Fertility problems also may develop. Fortunately, effective treatments are available. Causes of EndometriosisThe exact cause of endometriosis is not known. However, possible causes include the following: Your immune system may not be getting rid of endometrial cells outside of the uterus like it should. Heavy bleeding or an abnormal structure of the uterus, cervix, or vagina causes too many endometrial cells to go up through the fallopian tubes and then into the belly. (This is called retrograde menstruation). Blood or lymph fluid may carry endometrial cells to other parts of the body. Or the cells may be moved during a surgery, such as an episiotomy or a cesarean delivery. Cells in the belly and pelvis may change into endometrial cells. Endometrial cells may have formed outside the uterus when you were a fetus. It may be passed down through families. When to Call Your DoctorIf you develop sudden, severe pelvic pain, call your doctor immediately. Call a doctor to schedule an appointment if: Your periods have changed from relatively pain-free to painful. Pain interferes with your daily activities. You begin to have pain during intercourse. You have painful urination, blood in your urine, or an inability to control the flow of urine. You have blood in your stool, you develop pain, or you have a significant, unexplained change in your bowel movements. You are not able to become pregnant after trying for 12 months. Treatment OptionsThere is no cure for endometriosis, but treatment can help with pain and infertility. Treatment depends on how severe your symptoms are and whether you want to get pregnant. If you have pain only, hormone therapy to lower your body’s estrogen levels will shrink the implants and may reduce pain. If you want to become pregnant, having surgery, infertility treatment, or both may help. Not all women with endometriosis have pain. And endometriosis doesn’t always get worse over time. During pregnancy, it usually improves, as it does after menopause. If you have mild pain, have no plans for a future pregnancy, or are near menopause (around age 50), you may not feel a need for treatment. The decision is up to you. MedicinesIf you have pain or bleeding but aren’t planning to get pregnant soon, birth control hormones (patch, pills, or ring) or anti-inflammatories (NSAIDs) may be all that you need to control pain. Birth control hormones are likely to keep endometriosis from getting worse. If you have severe symptoms or if birth control hormones and NSAIDs don’t work, you might try a stronger hormone therapy. Besides medicine, you can try other things at home to help with the pain. For example, you can apply heat to your belly, or you can exercise regularly. SurgeryIf hormone therapy doesn’t work or if growths are affecting other organs, surgery is the next step. It removes endometrial growths and scar tissue. This can usually be done through one or more small incisions, using laparoscopy. Laparoscopy can improve pain and your chance for pregnancy. In severe cases, removing the uterus and ovaries (hysterectomy and oophorectomy) is an option. This surgery causes early menopause. It is only used when you have no pregnancy plans and have had little relief from other treatments. As OB/GYNs, we specialize in protecting your fertility and providing treatment to relieve physical suffering. Call today for an appointment at 770.720.7733 or schedule an appointment online.
Dr. Litrel addresses endometriosis in this Q&A session. Learn its symptoms, how it’s diagnosed and available treatment options.

Our Facebook Winter Baby Contest is ON! Enter your baby photos (ages 0-24 months) for a chance to win some great prizes and perhaps more importantly, bragging rights! To enter from your computer, simply go to our Facebook page. To enter from a mobile device such as your phone or tablet, click here! Contest runs from January 15th through January 29th! Prizes include: Grand Prize (TWO WINNERS): 16″x20″ Print on Canvas (to display those beautiful photos!) 2nd place: $25 Johnny’s Pizza gift certificate 3rd place: $25 Johnny’s Pizza gift certificate 4th place: Bojangle’s Picnic Pack 5th place: Chick-Fil-A basket with gift cards Can’t wait to see your most adorable winter baby photos! 🙂

Dealing with infertility can be one of the most stressful situations you’ll ever have to deal with. Not only are you struggling with your feelings, but you often have to field never-ending questions from family and friends. How to Handle ‘The Question’ So how do you handle baby questions when you’ve been struggling with infertility? Have an Answer Ready Talk with your husband or partner beforehand about how you’re going to handle these sensitive questions. Having a plan will make you feel much more at ease when it happens. Skip the Details There’s no reason you have to tell anyone you’re struggling to have a baby. Keep it vague so when you’re asked when you’re going to have kids, just reply, “Well, we hope to someday.” Then quickly ask them a follow up question that has nothing to do with babies. Use Humor There’s a reason some of the most tragic people in history have been so funny. They learned to use humor to deflect their real feelings so doing this when you’re asked uncomfortable questions can work wonders. So when they ask you when you’re going to have a baby, you can respond with, “Baby? Baby what? Baby dog? Baby cat?” Then just laugh it off. They’ll likely get the hint and change the subject. Believe in Good Intentions Most people have good intentions and are genuinely interested in your life and they’re really not trying to make you uncomfortable. The thing is, most people who haven’t struggled with infertility have no idea what a sensitive subject it can be. Try to keep that in perspective. Conversations about when you’re going to have a baby can either make or break your mood. But by taking some of these steps, hopefully you’ll feel more comfortable and be better able to enjoy those baby questions.

You’re having a baby! Yipee!! Oh but wait, that means doctor’s appointments. But after that initial joy, reality sets in and you realize you’re in store for a lot of appointments. And exams. And blood being drawn. Ugh. But fear not, we’re here to help you with real issues expectant moms face when visiting the OB. The Wait! Oh, the Wait! You booked your appointment and what happens? You sit in the waiting room for what seems like days. No one likes waiting but thank goodness, most of us now have smart phones to help distract us. So to help pass time, whip it out and play a game of Words with Friends, check your friends’ status updates or get caught up on your work emails. Whatever it is, these distractions can be a huge help in passing the time. Book Your First OB Appointment Early Sure, an extra hour of sleep is awesome but if you book your appointment early in the day, you’re more apt to be seen quicker than if you booked a later appointment. Why? Because an early appointment means the office is less likely to be running behind. But what happens if an early appointment isn’t available? Call ahead to see if things are running on time. The receptionist may just tell you it’s okay to show up a little later. Just be sure to triple check how late you can show up as you’d hate to lose your spot altogether! Go to Your Happy Place The dreaded exam. Nobody likes it. After all, you’re showing your most intimate parts to a near stranger and you can’t help but wonder if you’re “normal” or if you groomed well enough, etc., etc. Oh, the things that run through our minds when we’re on that exam table! Some of us joke to the point of embarrassing ourselves (yours truly), while others think of anything other than the task at hand. But just remember this, while it’s the first time in months that your legs have been in stirrups, it’s the umpeteenth time your doctor has seen the same parts just that week. And as any OB will tell you, they’ve seen every size, shape and form and they certainly aren’t passing judgment. They’re simply there to help you with your health concerns. Blood Work Being probed and having your blood drawn isn’t exactly on anyone’s bucket list. But there are a few things you can do to help alleviate the discomfort. Start by talking to your doctor before the exam. Ask them what you can expect to feel before they start. Just knowing what to expect can take a lot of the fear and surprise out of it. And the less tense you are, the less discomfort you will feel. Another great tip is listening to music on your iPod, taking deep breaths or visualizing a favorite vacation. When you’re having your blood drawn, look away and don’t be afraid to turn into a Chatty Cathy. These tricks will definitely help take your mind off of things. Ask Those Questions If you ever feel like your doc breezes in and out before you even have a chance to ask one question much less the list of questions you had in mind, you will definitely leave your appointment frustrated and worse than that, without the information you need. To help ensure you get what you need out of your appointment, have a list of your questions in hand when the doctor enters the room and just start asking! And please know, it’s highly likely that your doctor isn’t even aware that you’re feeling rushed. She just knows that she has a lot more patients to see and is doing her best to keep on schedule. To get more time next time, ask if you can schedule a longer appointment. Just be sure to ask if you’ll be billed extra and if insurance will cover it. Birth Plans: More Like a Wish List You’ve put a ton of time into creating the perfect birth plan and you’re so excited to show your doctor how invested you are and what happens? She barely glances at it. What?! Before you get upset, try looking at it from the doc’s point of view. If everyone handed her a novel of a birth plan, she’d never get around to seeing her patients. So what to do? Make a list of bullet point items and discuss them with her. And make sure you prioritize and touch on the deal breakers without focusing so much on your “wish list”. This will help ensure that you’ll be heard and your doc is more apt to take your preferences seriously. Hopefully these tips will make your next OB visit a little more pleasant. To schedule your appointment, please call us at 770.720.7733 or simply schedule an appointment online.

Dr. James Haley shows what a sling looks like and explains how it’s used to cure a leaky bladder. Read his corresponding article.
Dr. Litrel offers tips to avoid getting an STI and what to do if you suspect you have one. Watch more GYN Problems videos below

A miscarriage was not what Ashley expected to happen with her first pregnancy. Here, she shares her emotional story. After many years, Ashley and her husband became pregnant, and they were ecstatic. However, that excitement was short lived as it ended up being a long series of doctor’s visits and Ashley getting her blood drawn every three days. It was not how she envisioned her first pregnancy. Unfortunately, Ashley’s pregnancy resulted in a miscarriage, and it was a heart wrenching process. “My husband, Jesus and you helped me through a difficult miscarriage. You were great. Every time you saw me, you prayed for me,” Ashley tells Dr. Litrel. Ashley’s Advice for Others Suffering from Miscarriage Dr. Litrel asked Ashley if she had any wisdom to share with others who are going through — or have gone through — a miscarriage. Ashley said, “It’s okay if you don’t want to be around your pregnant friends. Allow yourself to hurt and hurt deeply. Give yourself permission to be angry. Open up your heart to God.” Pregnant Again! Ashley did become pregnant after her miscarriage and she’s over the moon. As Dr. Litrel showed her the ultrasound, she couldn’t hide her joy as she exclaimed, “Go little heart, go!”

We understand that discussing heavy bleeding can be embarrassing to talk about. You may not even realize that what you experience each month is abnormal because your periods are normal to you. However, it is critical to recognize what defines heavy bleeding as it may be a symptom of other issues that require further medical attention. What Are the Causes of Heavy Bleeding? There are many factors that can cause heavy bleeding. In young women who have just started having regular periods as well as premenopausal women, heavy bleeding is often due to a hormonal imbalance between the estrogen and progesterone levels. This hormonal imbalance may also be caused by a malfunction of the ovaries. Fibroids may also be a cause of heavy bleeding. Fibroids are non-cancerous tumors inside the uterus, they are most common in women who are within their peak child-bearing years as this is when hormone levels are at their highest. What Are the Symptoms? The symptoms may seem difficult to identify because they may seem normal to you. The average period only produces about two to three tablespoons of blood and lasts about four to five days, if you are soaking through a tampon or pad hourly for many consecutive hours you may have heavy bleeding. Other symptoms include severe cramps, periods that last longer than seven days, and passing clots larger than a quarter. You may also experience fatigue and shortness of breath. These symptoms are signs of anemia which can be caused by severe blood loss. Are you still unsure about your symptoms? Take our Heavy Bleeding Quiz. How is Heavy Bleeding Treated? Treatments vary depending on what is causing the heavy bleeding. Options may include simple over the counter medicines, low-dose birth control pills or hormone therapy. In some cases, your bleeding can be treated with ablation. Ablation is a new treatment that can be done in our office in about ten minutes. Check with your physician to see which is right for you. Talk to Your Doctor There is no reason your life should be on hold each and every month. If you find that your monthly period is taking a toll on your lifestyle, schedule an appointment to talk to your physician about treatment options and getting your life back on track without monthly interruptions. Or, call us at 770.720.7733.

If you’re pregnant, a flu shot is your best protection against serious illness from the flu. Flu is more likely to cause severe illness in pregnant women than in women who are not pregnant. Changes in the immune system, heart and lungs during pregnancy make pregnant women more prone to severe illness from flu, which can lead to hospitalization or even death. A pregnant woman with the flu also has a greater chance of serious problems for her unborn baby, including premature labor and delivery. The Flu Shot is the Best Protection Against Flu Getting a flu shot is the first and most important step in protecting against flu. When given during pregnancy, the flu shot has been shown to protect both the mother and her baby (up to 6 months old) from flu. The flu shot is safe to get at any time while you are pregnant, during any trimester. (The nasal spray vaccine should not be given to women who are pregnant.) An additional way to protect the baby is for all of the baby’s caregivers and close contacts (including parents, brothers and sisters, grandparents, and babysitters) to get vaccinated against the flu. When to Receive the Flu Vaccine It is particularly important that women who are or will be pregnant during the flu season receive an inactivated flu vaccine as soon as it is available. The inactivated flu vaccine can be given to women at any point during their pregnancy. Live, attenuated flu vaccine is available as an intranasal spray and is not recommended for pregnant women, but is safe for use in women in the postpartum period. In the United States, the influenza season typically occurs from October through May. The preponderance of data overwhelmingly demonstrates the safety of flu vaccination during pregnancy. The Flu Shot is Safe for Pregnant Women Flu shots are a safe way to protect pregnant women and their unborn children from serious illness and complications of flu, like pneumonia. The flu shot has been given to millions of pregnant women over many years. Flu shots have not been shown to cause harm to pregnant women or their babies. It is very important for pregnant women to get the flu shot. Early Treatment is Important for Pregnant Women If you get sick with flu-like symptoms, call your doctor right away. If needed, the doctor will prescribe an antiviral medicine that treats the flu. Having a fever caused by flu infection or other infections early in pregnancy can lead to birth defects in an unborn child. Pregnant women who get a fever should contact their doctor as soon as possible. More Facts to Support the Importance of Flu Shots The Center for Disease Control and Prevention (CDC) recommends that all adults get vaccinated for influenza. This is especially true for woman who are pregnant. According to a study conducted by American College of Obstetricians and Gynecologists (ACOG), the number of pregnant women who are vaccinated has gone up since last recorded in 2010. However, it is still important that this number continues to increase. If a woman is – or may become pregnant – during the height of the influenza season, it is critical that she get vaccinated as quickly as possible. Flu season is usually between October and May. It is recommended that pregnant women receive the inactivated flu vaccine as it has been proven to be safe throughout the gestation period. Different immunization options are available for women who are postpartum so be sure to check with your physician about which options are right for you. In addition to the benefits and protection provided by being vaccinated, a recent randomized trial found that the children of vaccinated women had fewer instances of getting the flu as well as fever and respiratory illness as opposed to children whose mothers were not vaccinated. Studies have also shown that some of the antibodies may be passively acquired by the baby in utero when pregnant women are vaccinated. This helps babies fight any threat to influenza after they are born. Newborns up to six months of age cannot receive the influenza vaccine. Where to Receive the Flu Vaccine At Cherokee Women’s Health Specialists, we are committed to making sure you are well-informed so you may make the healthiest decisions for yourself and your families. To make it as easy as possible for you to receive a vaccination, following is a list of places in the Canton and Woodstock areas that offer flu shots: CVS Walgreens Publix

Urinary incontinence is not an uncommon problem. In fact, 1 in 5 women struggle with it. Incontinence itself is not a disease but rather an indication that there is something else going on inside the body. It’s important to speak to a doctor to ensure that your incontinence is not a symptom of a more serious medical issue. Incontinence can be caused by various factors. Some of your day-to-day activities could be causing what is known as temporary urinary incontinence. Different foods, drinks, diuretics and even medication may be causing you to feel a seemingly constant urge to use the bathroom. If you regularly consume caffeine, artificial sweeteners, sodas, alcohol or highly acidic beverages, this may also be a factor. Temporary urinary incontinence may also be a symptom of a urinary tract infection or constipation. All forms of incontinence are treatable. Pelvic floor exercises are a great way to help rebuild the strength in those critical muscles after childbirth. In addition, there are several prescription medicines and minimally invasive surgeries available. Be sure to talk to your physician about which options are right for you and your needs. Persistent urinary incontinence is a side effect of many natural changes women experience. From childbirth to aging, there are several natural factors that can affect the severity and frequency of your symptoms. The muscles surrounding your bladder and pelvic floor experience many changes throughout the course of your life. When women are pregnant and then deliver vaginally, bladder muscles are weakened and there is also a possibility for nerve damage. As women continue to age, bladder muscles get weaker. When a woman reaches menopause, estrogen levels begin to decrease. Estrogen is responsible for maintaining the health of your bladder and urethra tissues. As the health of those tissues decline, this can add to the severity of a woman’s incontinence. Preparing for Your Appointment In preparing for your appointment to address urinary incontinence, keep a list of your diet, medications and how many times you are using the restroom. This added information will be very helpful to your physician in addressing your symptoms. Women are affected by incontinence at all stages of life. It’s important to not let it go untreated and to understand that you are not alone. At Cherokee Women’s Health Specialists, we’re committed to giving you the answers and treatment you need while also making sure that you are comfortable. To make an appointment, please contact us here.
