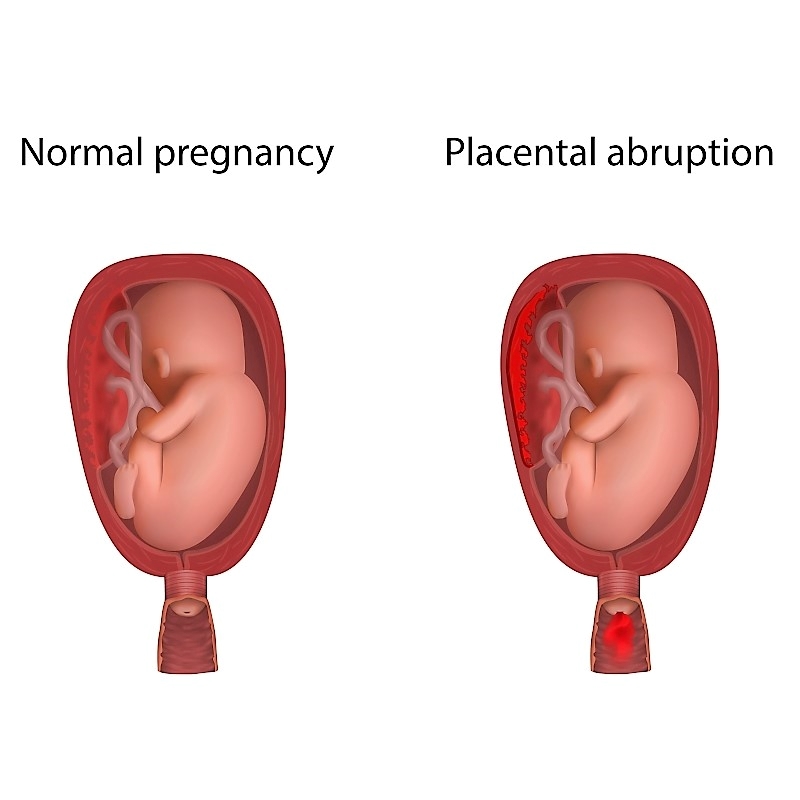
By James P. Haley, MD, FACOG, FPMRS As an OB/GYN for over 30 years now, I feel the need to speak out strongly against home births. I have certainly delivered my fair share of babies, and what a privilege it has been to witness one of God’s greatest miracles, thousands and thousands of times in my career. I am honored to have shared with so many families one of the most special and intimate moments in their lives. One of my greatest blessings was being able to deliver my two children – memories that my wife and I will always treasure. Home Births Come with Extreme Risks There is a growing trend in OB that has me greatly concerned, and I feel the need to speak out strongly against it. It is the growing popularity of pre-planned home births. The trend seems to be gaining some momentum, and approximately 1-2% of all U.S. births are now delivered at home. According to recent statistics, that number is rising. The truth is, there are extremely serious risks involved with attempting to deliver at home, and women and their families need to be aware of these dangers. We have come a long way in modern medicine, especially in the field of Obstetrics. In the early 1900s when home births were the reality, one in ten babies died at birth. Sadly, many of these infants suffered trauma at birth resulting in complications such as seizures, paralysis, or brain damage. Death was common and the mother’s life was always at risk, as up to 1 in 100 mothers died giving birth. As OB/GYNs, We Have Seen it All With advances in modern technology, it is alarming as to why many would consider delivering at home without immediate access to a hospital. The American College of Obstetrics and Gynecology recommends that babies be delivered in hospitals. They want everyone to know that babies born at home are twice as likely to die, and three times more likely to have neurologic dysfunction or brain damage. The American Academy of Pediatrics concurs with ACOGs opinion and agrees that hospitals are the safest place to give birth. Even today, giving birth is one of the most dangerous things a woman can do. In the U.S., it is the sixth most common cause of death among women ages 20-34. These statistics are very troubling, and much research and study is being done to continually lessen the maternal death rate. OB/GYNs know with absolute certainty the risks of childbirth and the possible dangers that can go wrong. We have seen it all and there are often complications that can arise within a few minutes that no one saw coming. It is very humbling; and we have all seen multiple times where, had the patient not been in the hospital — in labor, being monitored and under close observation — the baby would have died. It happens quite frequently. Usually, with proper prenatal care, we can predict problems and future complications, treat them, monitor closely, and be prepared for those potential complications at birth. “I have personally seen hundreds of babies that would have died, had the patient not been at the hospital at that moment. After moments like that, you not only see the amazing hand of God, but also greatly appreciate the advances in modern medicine. And you are grateful you were there exactly at that moment – and in a hospital.” – Dr. James Haley However, childbirth as we know doesn’t always go smoothly or as planned. Occasionally, a medical crisis arises that causes the entire team of doctors and nurses to jump into immediate action, work together like nothing you’ve ever seen — all to get that baby out in 2-3 minutes to save its life — while also trying to take care of the mother and keep her safe. Common Problems that can Occur Throughout Pregnancy, Delivery and After: Following are just a few problems that can occur throughout a woman’s pregnancy, delivery and postpartum. Gestational diabetes High blood pressure Preeclampsia Preterm labor Anemia Infections Breech position Fetal distress Premature rupture of membranes Placenta problems Placental abruption Prolonged labor Perinatal asphyxia Shoulder Dystocia Excessive bleeding Malposition Placenta previa Cephalopelvic disproportion Uterine rupture Rapid labor Oxygen deprivation Umbilical cord prolapse Umbilical cord compression Velamentous Cord Insertion Chorioamnionitis (Infection) Fetal macrosomia (Extra-large infant) Postpartum hemorrhage (Bleeding) Postpartum preeclampsia Why Take the Risk of a Home Birth? Women that consider home birth typically want fewer medical interventions, they want to enjoy the comforts of home, enjoy a more satisfying and natural birth, and have control over all aspects of the birthing process. These are all valid wants and desires, and it is understandable how people are driven to choose this route. If you have had a home birth and all has gone well, that is great. However, I wouldn’t push your luck and do it again. You have dodged many, many bullets. There are medical offices and midwives that attempt to facilitate and “ensure” the safety of a home birth. Hospitals are nearby, and women are told that if complications arise, they can abort the plan and head to the hospital. In fact, the latest statistic shows that approximately 30-35% of planned home births end up delivering at the hospital after all. But at what cost? Do they make it in time? These actual statistics don’t often end up in the “home delivery” category. Once they are sent to the hospital, they are counted as hospital deliveries, so we don’t truly know if they had complications or even the worst possible outcome occurred. Working in the hospital and a busy medical practice, I have sadly seen some tragic outcomes. Just a few weeks ago, I personally saw a patient that had been going to the type of practice that is more “natural” and encourages and oversees home births. The mother suspected a problem and was referred to me for an evaluation. “Unfortunately, I confirmed their greatest fear, that the